I'm a physicist. My default mode is to quantify things, to ground arguments in data rather than intuition. So when people ask me why the Appalachian Radiotheranostics Coalition exists, why this geography, why now, why theranostics, my answer isn't a story. It's a set of numbers that, once you see them, you can't unsee.
Here's what the data actually say.
Appalachia Has a Cancer Problem That Isn't Improving at the Same Rate as the Rest of the Country
Across the United States, cancer mortality rates have been falling since 1991. That's genuinely good news, a product of better screening, earlier detection, and improved therapeutics. But that progress has not been evenly distributed.
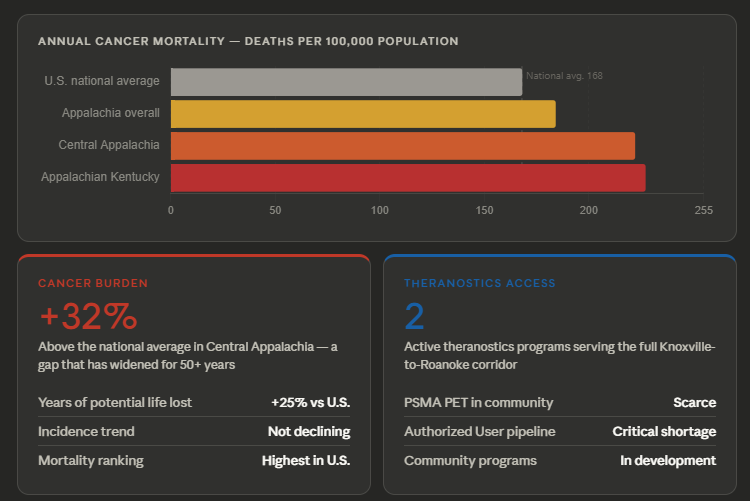
The Appalachian region, which spans 423 counties across 13 states from southern New York to Mississippi, carries a cancer mortality rate of 184 per 100,000 population which is 10% above the national average. Central Appalachia fares worse still, at 222 per 100,000, a rate 32% higher than the national figure. In Appalachian Kentucky, the number climbs to 227 per 100,000 that puts that region 35% above the national average.
Perhaps more telling than the absolute numbers is the trend. Cancer incidence has declined in every U.S. region except rural Appalachia. Rural Appalachians also have lower 3-year and 5-year cancer survival rates than their urban non-Appalachian counterparts. And when you look at years of potential life lost, a measure that captures premature death, the Appalachian rate runs 25% higher than the national average.
The gap isn't closing. In Appalachian Kentucky, the cancer mortality disparity has been widening for over 50 years—not shrinking.
Hudson et al., Journal of Rural Health, 2024A 2025 analysis published in the Journal of the American College of Surgeons, using the most current county-level data, confirmed that while progress is happening, cancer incidence and death rates in Central Appalachia remain substantially higher than anywhere else in the country. And the region dies disproportionately from cancers that are detectable early. That strongly suggests to you that this isn't purely a biology problem. It's an access problem.
The Therapies Exist. The Access Does Not.
Here's the tension at the heart of what we're doing with ARC: we now have FDA-approved targeted radiopharmaceutical therapies (177Lu-PSMA-617 for metastatic castration-resistant prostate cancer, 177Lu-DOTATATE for neuroendocrine tumors) that are demonstrably effective. The Phase 3 VISION trial established the clinical case for lutetium PSMA therapy. The evidence base is solid.
And yet, a comprehensive situation analysis by the Health Policy Partnership found that the U.S. healthcare system faces substantial structural barriers to delivering these therapies at scale, and those barriers fall disproportionately on community and rural settings.
What does that look like in practice? The Health Policy Partnership summarizes it well: dedicated RLT treatment suites remain in short supply. PSMA PET imaging, required for patient selection, is less available in community settings. Multidisciplinary team coordination is inconsistent. Billing and coding for these therapies is complex enough that many centers miss reimbursement they're entitled to, creating poor first experiences that discourage adoption. And without referring providers who understand these options, eligible patients never make it into the pipeline in the first place.
The primary barrier to theranostics access in community settings isn't hardware or radiopharmaceutical supply. It's a trained workforce and referring providers who know where they can send patients.
The Workforce Gap Is Real...and Growing
Delivering radioligand therapy requires an Authorized User, a physician certification that's specific, credentialed, and not interchangeable with general oncology training. The Radiology Review put it plainly: Authorized Users are on track to become among the most sought-after specialists in oncology, and the pipeline producing them is far too thin to meet accelerating demand. Pluvicto crossed $1 billion in sales in the first nine months of 2024. Demand is real and growing fast.
A Lancet Oncology analysis on nuclear medicine workforce trends frames the problem globally but applies with particular force in rural regions: providing education, experience, and expertise in theranostics to the nuclear medicine technologist community is an enormous challenge, especially given worldwide shortages of trained professionals. In the U.S., the number of nuclear medicine physicians graduating from training programs has not kept pace with clinical demand. That problem was already visible before the theranostics boom and is now compounding.
This matters especially along the Appalachian corridor. Academic medical centers with established theranostics programs have the infrastructure, the teams, and the experience. Community hospitals in the corridor serve patients who would otherwise need to travel hours to access these therapies, yet most don't have dedicated theranostics programs. What they do have is nuclear medicine departments, SPECT/CT systems, and staff who could be trained. What's needed is practical, competency-based education designed for community settings, not academic curricula adapted after the fact.
At smaller centers, the multidisciplinary team may only consist of the referring oncologist, nuclear medicine coordinator, and scheduler. Telemedicine allows specialists from large centers to consult, but someone at the community level has to know enough to ask.
Mittra et al., Establishing a Robust Radioligand Therapy Program, PubMed 2024Why the Corridor. Why ARC.
The Knoxville-to-Roanoke corridor wasn't chosen arbitrarily just because we live here. It was chosen because the data justified it. NCI maps of cancer mortality by county show elevated rates concentrated precisely in this swath of central Appalachia: Ohio, Kentucky, Virginia, West Virginia. The corridor has two anchor institutions, UT Medical Center in Knoxville and Carilion Clinic in Roanoke, that are already running active theranostics programs. Between them are community hospitals and cancer centers whose providers are increasingly aware these therapies exist and working to ramp up, but aren't yet equipped to fully deliver or coordinate them.
ARC exists to close that gap. Not by pulling patients to academic centers, but by bringing training, resources, and infrastructure to the providers already serving these communities. The four workshops we're running this year, the online resource hub, the curriculum we're building: all of it is designed with one question in mind. What does a nuclear medicine professional or oncologist at a community hospital in southwestern Virginia actually need in order to use these therapies?
The data make the case for urgency. The geography makes the case for this corridor specifically. And the workforce gap makes the case for why education, not just equipment or supply chain, has to be the intervention.
Prostate cancer is common in this region. Neuroendocrine tumors don't discriminate by zip code. The patients who need these therapies are already here. The question is whether the knowledge to deliver them will be.
What's Your Take?
If you're working in nuclear medicine or oncology outside a major academic center, I'd genuinely like to know: what's the biggest barrier you're seeing to theranostics adoption at your site? Is it referring provider awareness? Staffing? Reimbursement complexity? Something else entirely? Drop your answer in the comments. This is exactly the kind of on-the-ground intelligence that shapes what ARC is building.
References
- FDA Conversations on Cancer – Cancer Disparities in Appalachia (July 2023)
- Zahnd & Ganai. Cancer Disparities in Rural Appalachia: Incidence, Early Detection, and Survivorship. PubMed, 2016.
- Hudson et al. Cancer Disparities in Appalachian Kentucky. J Rural Health, 2024.
- Burus et al. Examining Geographic Disparity: Variation in Cancer Outcomes within Appalachia. JACS, 2025.
- Appalachian Regional Commission. Health Disparities in Appalachia: Mortality Domain.
- Pharmacy Times. Patients in Appalachia Face Unique Disparities, Obstacles to Care.
- NCI. Addressing Cancer Disparities in Appalachia.
- The Health Policy Partnership. Health System Readiness for Radioligand Therapy in the US: Situation Analysis Report. 2021.
- Avalere Health. Patients Are Ready for Radioligand Therapy, But Is Our Healthcare System?
- Mittra et al. Establishing a Robust Radioligand Therapy Program: A Practical Approach for North American Centers. PubMed, 2024.
- Herrmann et al. Trends in Nuclear Medicine and the Radiopharmaceutical Sciences in Oncology: Workforce Challenges and Training in the Age of Theranostics. Lancet Oncology, 2024.
- The Radiology Review. Radioligand Therapy: Transforming Cancer Care Amid Workforce Shortages.